
Dr. Maxwell Nartey
Professor of Symptometric Science, American School of Symptometry, NFP
The wonders of Symptometry
To some women, if Symptometry cannot help them avoid surgery, then, why contact Symptometry or have symptometric services?
The truth is, for many years, Symptometry did not have excellent hydrolyzers, and oxidizers. Now, it has them. Also, it did not have the molecules that enable a person who cannot thoroughly digest saturated fat to digest it while staying away from many sources of saturated fat. Now, it has these molecules. What a difference ten years make!!!
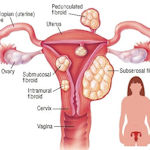
If the fibroids are small or medium in size, Symptometry’s scientific eating and living, as well as its hydrolyzers and oxidizers can, over time, shrink the fibroids. However, if the fibroids are huge and massive, Symptometry can free float the fibroid, but it will take over two years to liquefy it. This is why surgery would be the recommended option.
Another truth is, not all surgeons are good. The best surgeons for myomectomy have been women who are also gynecologists, and have children. They understand the importance of saving the reproductive organs of a woman who has fibroids, even if that woman is in her fifties or sixties.
In March 2021, a woman who had a huge fibroid that weighed over 15 lbs. underwent ELAM (exploratory laparotomy abdominal myomectomy), and the 90-minute procedure was amazingly successful. This procedure allowed the woman to save all her reproductive organs. This is better than Amazing.
Before the procedure, Symptometry used a scientific method to prepare her entire body for the procedure.
After the procedure, Symptometry gave her 1) hydrolyzers to liquefy the anesthetic drugs that were in her eleven systems 2) enhancers of granulation to help her heal faster; and 3) enzyme builders to accelerate the production of endorphins, substance P, enkephalin and cortisol. As a result, she had minimal pain, and no inflammation.
More importantly, there was no uterine hemorrhaging. The surgeon was pleasantly surprised that there was no uterine hemorrhaging because usually, there is a whole lot of uterine hemorrhaging.
The surgeon was not aware that the woman on whom she operated had help behind-the-scenes. The provider of this behind-the-scenes help was Symptometry.
There will come a time when surgeons and doctors of Symptometry would work together for the benefit of mankind. That time has not yet come, but it will.
See the photograph of the fibroid that was taken out of the woman in question in March 2021 through ELAM. It was on the table for all to see. Part 4 of this series is the case study, which must be read because of its extreme significance
CASE STUDY
HISTORY
Active 37-year-old woman, 5’4”, 135lbs, no prior history of abnormal growths, no alcohol or tobacco usage, regular aerobic exercise, vitals within normal range (except HCL at 133), menstrual cycle lasts 5-7 days (without cramps)
DIAGNOSIS
 In Feb ’21 – ultrasound and CT scan reveal abdominal mass approximately 10 inches in length but no clear image of its origin.
In Feb ’21 – ultrasound and CT scan reveal abdominal mass approximately 10 inches in length but no clear image of its origin.
Due to size, location and assumed weight, the primary physician suspected the mass was a malignant tumor and stemming from the left ovary.
Gynecologist-oncologist assumed the mass was a ‘fibroid’ but was unable to define the mass based on imagery and they discussed invasive and non-invasive treatment options.
CHALLENGE
The abdominal mass had exceeded probability of success with non-invasive treatment options due to size and location. The remaining option was, major surgery, but a major surgery increased the probability of subject suffering from any combination of the following ‘worst-case scenarios’: 1) hysterectomy 2) extraction of one or both ovaries 3) blood transfusion (due to excessive blood loss) 4) hemorrhaging of the uterus 5) infertility 6) inability to conceive or birth offspring vaginally.
SOLUTION
Symptometry has hydrolyzers that will force the fibroid to ‘free-float’ in the abdominal cavity, which allows a skilled surgeon to extract it through a single-surgical incision. The surgical procedure is called a myomectomy but there are different types – for instance, this subject received an ELAM (exploratory laparotomy abdominal myomectomy) due to the nature of the mass compared to the size of the subject.
A Symptometry-approved diet was enforced well in advance. However, two weeks prior to the surgery, Symptometry provided the patient with molecules to be taken daily in a bid to increase oxygen in the blood and strengthen blood vessels – in hopes of decreasing the probability of excessive blood loss.
OUTCOME
In March ’21, the 90- minute procedure was amazingly successful. After the procedure, Symptometry gave the subject 1) hydrolyzers to liquefy the anesthetic drugs and their lasting effects on the body 2) enhancers of granulation to expedite healing; and 3) enzyme builders to help her produce endorphins, substance P, enkephalin and cortisol faster. As a result, her pain was manageable, with no inflammation – confirming no need for pharmaceutical drugs during recovery.
HIGHLIGHTS
The subject did not suffer from any ‘worst-case scenarios.’ The surgical team was shocked at the ease of the extraction. However, they were not aware that the patient had ‘behind-the-scenes help’ from Symptometry.
It was Symptometry and the Creator that made this operation successful. Amazing!!!
Integrative medicine is becoming widely accepted – soon it will become the norm. Depending on when a subject discovers Symptometry is the difference between preventing a surgery and creating a miraculous success story after a surgery. Read the details of the case study on this uterine fibroid; and see the photograph of the fibroid that was taken out in March 2021 through ELAM.
© Copyright 2021, The American School of Symptometry, NFP. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system without the written permission of The American School of Symptometry, NFP. Library of Congress copyright number Txu 1-621-370, Washington D.C.
 Previous Post
Previous Post